What is Pre-implantation Genetic Testing for Aneuploidies (PGT-A)?
At Sunfert, we offer Pre-implantation Genetic Testing for Aneuploidies (PGT-A) as a genetic screening tool to examine embryos created through IVF before they are transferred to the uterus.
PGT-A helps us identify whether an embryo has the correct number of chromosomes. Chromosomes carry genetic information, and a healthy embryo typically contains 46 chromosomes arranged in 23 pairs.
How are Embryos Screened using Advanced Genetic Technology?
To perform PGT-A accurately, we use a technology called Next-Generation Sequencing (NGS) at Sunfert. This is a top-notch advanced genetic testing technology in the industry that allows us to examine the DNA of an embryo in detail, helping us determine whether it has the correct number of chromosomes.
During the PGT-A process, a few cells are carefully taken from the embryo and analysed using NGS. This technology can screen all 23 pairs of chromosomes at once with high precision, allowing us to identify embryos that are chromosomally normal as well as those with chromosomal abnormalities. By selecting embryos with the correct chromosomal count, PGT-A helps improve the chances of successful implantation, supports a healthier pregnancy, and reduces the risk of miscarriage for patients undergoing IVF.
What are Chromosomal Abnormalities?
A normal embryo has 23 pairs of chromosomes. Chromosomal abnormalities occur when there is an extra chromosome, a missing chromosome, or a structural imbalance in the embryo. These abnormalities may increase the risk of:
- Implantation failure
- Miscarriage
- Genetic disorders
By screening embryos before transfer, we aim to select embryos with the correct chromosomal count to improve the chance of establishing a healthy pregnancy.
Examples of Chromosomal Abnormalities
Some disorders that arise from chromosomal abnormalities include:
- Down’s Syndrome (Trisomy 21): caused by extra copy of chromosome 21
- Edwards’ Syndrome (Trisomy 18): caused by extra copy of chromosome 18
- Patau’s Syndrome (Trisomy 13): caused by extra copy of chromosome 13
- Turner Syndrome (Monosomy X): caused by a missing copy of chromosome X in female embryos
- Other numerical chromosomal abnormalities (aneuploidies) may lead to implantation failure or miscarriage
When combining IVF treatment with PGT-A, we can reduce the risk of transferring embryos with detectable chromosomal abnormalities.
Who Should Consider PGT-A?
We generally recommend PGT-A for individuals or couples who:
- are at an advanced maternal age
- have had recurrent miscarriages
- have experienced recurrent implantation failure
- have previously had a pregnancy affected by chromosomal abnormalities
- produce multiple embryos and want to prioritise chromosomally normal embryos
- wish to reduce the risk of transferring embryos affected by disorders such as Down’s Syndrome
At Sunfert, we assess each case individually to determine whether PGT-A is clinically appropriate for our patients’ fertility journey.
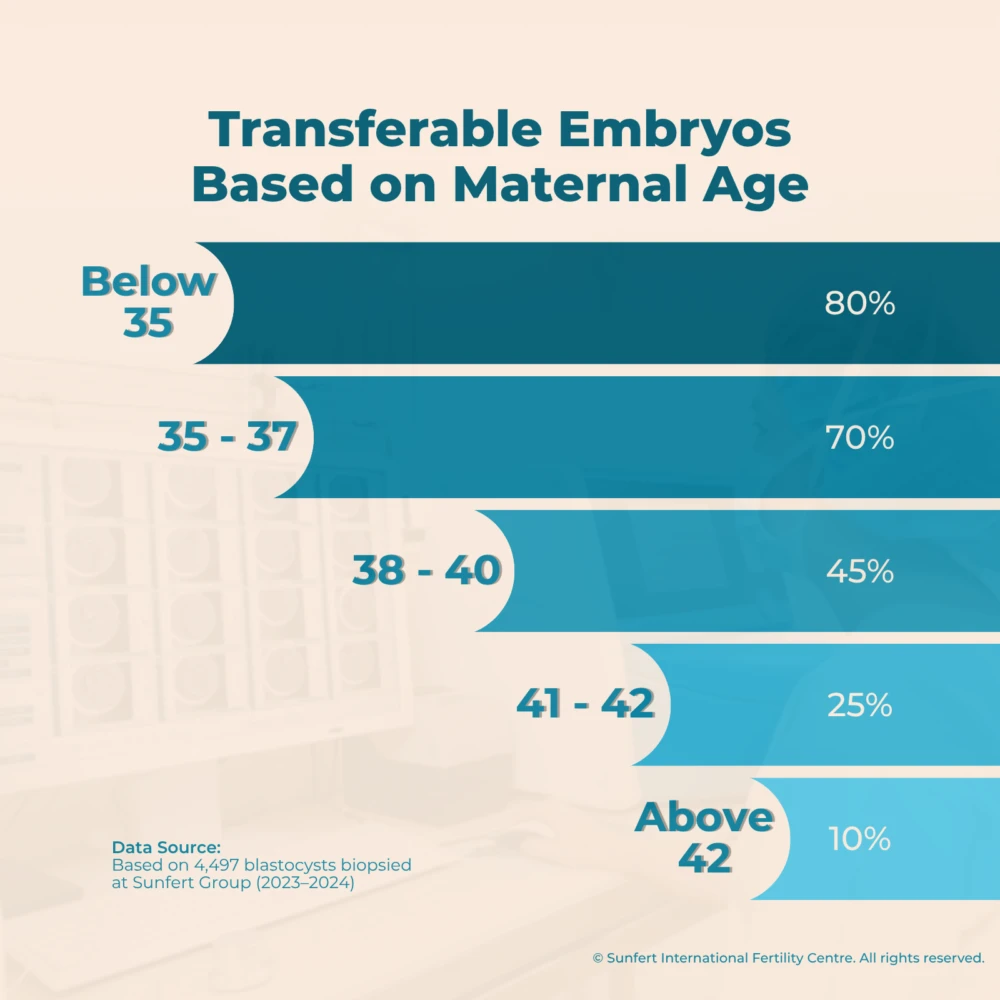
Our data and research at Sunfert shows that PGT-A benefits women of all age groups, especially those with advanced maternal age. As age increases, the number of transferable embryos decreases, and PGT-A can help identify the healthiest embryos for a higher chance of success.
The chart below is based on data from 4,497 blastocysts biopsied at Sunfert Group. The findings show that transferable embryo rates were highest among women below 35 years old, reaching up to 80%, while the transferable embryo rate among women aged 42 years old and above was approximately 10%.
Who Can Benefit from PGT-A?
PGT-A can benefit patients who want greater confidence in embryo selection before transfer.
We often see positive value for those who:
- are planning pregnancy at a later reproductive age
- want to minimise miscarriage risk linked to chromosomal abnormalities
- aim to increase the IVF treatment success rate with a more targeted, evidence-based embryo transfer plan.
For many patients, it provides reassurance by giving us additional genetic insight into the quality of their embryos.
Does PGT-A Improve IVF Success Rates?
Based on data collected from our patients, incorporating Pre-Implantation Genetic Testing (PGT) into IVF treatment improved IVF success rates and outcomes, including higher clinical pregnancy rates and implantation rates.
The comparison below shows the differences in clinical pregnancy and implantation rates between patients who underwent IVF with PGT and those who underwent IVF without PGT.
Sunfert Clinical Pregnancy Rate
| Age Group | Non PGT | PGT |
|---|---|---|
| <35 | 62.3% | 59.7% |
| 35 - 37 | 53.5% | 71.7% |
| 38 - 40 | 46.3% | 67.1% |
| >41 - 42 | 17.4% | 48.2% |
| Overall | 54.8% | 64.5% |
Sunfert Clinical Implantation Rate
| Age Group | Non PGT | PGT |
|---|---|---|
| <35 | 57.9% | 60.0% |
| 35 - 37 | 47.7% | 69.9% |
| 38 - 40 | 43.3% | 66.3% |
| >41 - 42 | 11.1% | 48.2% |
| Overall | 49.5% | 63.9% |
Notes:
- The Sunfert Clinical Pregnancy Rate and Implantation Rate (success rate) shown above were calculated based on data collected at Sunfert Bangsar South in 2024.
- In patients below 35, PGT is less frequently indicated. As a result, outcomes in this group are based on a smaller sample size, which may affect the observed clinical pregnancy rate.
Click here to learn more about Sunfert IVF Success Rate.
How is PGT-A Performed at Sunfert?
Step 1: IVF Treatment & Embryo Development
We stimulate the ovaries, retrieve the eggs, and fertilise them in our laboratory through IVF/ICSI.
The embryos are cultured until they reach the blastocyst stage (Day 5 or Day 6).
Step 2: Embryo Biopsy
Performed by our highly-trained embryologists or genetic scientists, a tiny cluster of cells is collected from the outer layer of the blastocyst (trophectoderm biopsy).
Step 3: Pre-implantation Genetic Testing for Aneuploidies
The biopsied cells undergo chromosomal testing using advanced genetic technology to determine if the embryo has the correct number of chromosomes.
The results are generated and shared with our patients and fertility specialists within 2 to 3 weeks.
Step 4: Embryo Selection and Transfer
Embryos identified as chromosomally normal (euploid) are prioritised for transfer in a subsequent cycle to improve the likelihood of a healthy pregnancy.
Mosaic embryos, which contain a mix of normal and abnormal cells, may be considered for transfer in selected cases following careful clinical evaluation and counselling.
Take the Next Step with Our Fertility Specialists
If you are facing fertility challenges, start with a consultation at Sunfert. We will guide you through your fertility journey with expertise and compassionate care.
Make an appointment with our Fertility Specialist today and take the next step toward your parenthood goals.
-
 Book a consultation
Book a consultationDato' Dr Wong Pak Seng
Founder of Sunfert Group & Fertility Specialist- Sunfert@Bangsar South
-
 Book a consultation
Book a consultationDr Eeson Sinthamoney
Group Medical Director & Fertility Specialist- Sunfert@Bangsar South
-
 Book a consultation
Book a consultationDr Lim Lei Jun
Medical Director (Sunfert Bangsar South) & Fertility Specialist- Sunfert@Bangsar South
-
 Book a consultation
Book a consultationDr Sumithra Devi Valiapan
Consultant Obstetrician, Gynaecologist & Fertility Specialist- Sunfert@Bangsar South
-
 Book a consultation
Book a consultationDr Haris Njoo Suharjono
Medical Director (Sunfert Kuching) & Fertility Specialist- Sunfert@Kuching
-
 Book a consultation
Book a consultationDr Evelyn Pang Mei Foong
Obstetrics, Gynaecology & Fertility Specialist- Sunfert@Seremban
-
 Book a consultation
Book a consultationDr Chong Jie Wen
Consultant Obstetrician, Gynaecologist & Fertility Specialist (Sessional)- Sunfert@Ipoh
-
 Book a consultation
Book a consultationDr Rohani Binti Effendy
Consultant Obstetrician, Gynaecologist & Fertility Specialist (Sessional)- Sunfert@Bangsar South
-
 Book a consultation
Book a consultationDr Leong Huey Yin
Clinical Geneticist (Sessional)- Sunfert@Bangsar South
What is Pre-implantation Genetic Testing for Aneuploidies (PGT-A)?
Pre-implantation Genetic Testing for Aneuploidies (PGT-A) is an advanced genetic screening technique used during IVF to assess whether embryos have the correct number of chromosomes before transfer.
A healthy embryo typically contains 46 chromosomes (23 pairs). By identifying chromosomally normal (euploid) embryos, PGT-A helps improve implantation rates and supports a healthier pregnancy outcome.
What is the main purpose of PGT-A in IVF treatment?
The primary purpose of PGT-A is to select embryos with the correct chromosomal number, which can:
- improve chances of successful implantation
- reduce the risk of miscarriage
- lower the likelihood of chromosomal disorders
This allows fertility specialists to make more informed, evidence-based decisions during embryo transfer.
What are common examples of chromosomal abnormalities detected by PGT-A?
Common chromosomal conditions include:
- Down’s Syndrome (Trisomy 21)
- Edwards’ Syndrome (Trisomy 18)
- Patau’s Syndrome (Trisomy 13)
- Turner Syndrome (Monosomy X)
PGT-A can detect these numerical abnormalities before embryo transfer, helping reduce associated risks.
What are the advantages of combining IVF with PGT-A?
Combining IVF with PGT-A offers several advantages:
- more precise embryo selection
- reduced risk of chromosomal abnormalities
- improved confidence during transfer decisions
- potentially shorter time to achieving pregnancy
This approach supports a more personalised and evidence-based fertility journey.
Is PGT-A necessary for every IVF cycle?
No, PGT-A is not required for every patient. Its use depends on factors such as age, medical history, previous IVF outcomes, and personal preferences.
A fertility specialist will advise whether PGT-A is appropriate based on individual circumstances.
If you are considering PGT-A to reduce the risk of chromosomal abnormalities, such as Down's Syndrome, you may discuss this option with your fertility specialist to receive personalised advice.
Who should consider PGT-A during IVF?
PGT-A is commonly recommended for individuals or couples who:
- are of advanced maternal age
- have experienced recurrent miscarriages
- have had repeated implantation failure
- previously had pregnancies affected by chromosomal abnormalities
- want to prioritise the most viable embryos
At Sunfert, we aim to ensure that any additional procedures are only advised when there is clear clinical benefit, so patients are not undergoing or paying for steps that are not necessary for their fertility journey and treatment.
Can younger patients benefit from PGT-A?
Yes. While PGT-A is especially beneficial for women of advanced maternal age, younger patients may also benefit by:
- improving embryo selection accuracy
- reducing time to pregnancy
- minimising the emotional impact of failed cycles
Clinical evidence suggests it can enhance decision-making across different age groups.
Can PGT-A guarantee a successful pregnancy?
No, PGT-A does not guarantee pregnancy. While it improves the selection of chromosomally normal embryos and increases the implantation rate, other factors such as uterine health, embryo quality, and overall medical conditions also influence the overall IVF success rates.
Does PGT-A improve IVF success rates?
PGT-A can improve IVF success rates by selecting embryos with the highest implantation potential. Benefits may include:
- improved implantation rates
- reduced miscarriage risk
- fewer transfer cycles needed
However, outcomes vary depending on individual patient factors.
How long does it take to get PGT-A results?
PGT-A results are typically available within 2 to 3 weeks after the embryo biopsy.
This timeframe allows for detailed genetic analysis and accurate reporting to guide the next step in the IVF treatment plan.
How does PGT-A work using advanced genetic technology?
PGT-A is performed using Next-Generation Sequencing (NGS), a highly precise technology that analyses all 23 chromosome pairs simultaneously.
The process involves:
1. biopsy of a few cells from the embryo
2. DNA analysis using NGS
3. identification of chromosomal abnormalities
This detailed screening enables accurate embryo selection prior to transfer.
Does PGT-A detect all genetic diseases?
No. PGT-A specifically screens for chromosomal abnormalities (aneuploidies) and does not detect single-gene disorders.
For inherited genetic disorder, required a different test called PGT-M (Pre-implantation Genetic Testing for Monogenic disorders).
Is embryo biopsy safe for the embryo?
Embryo biopsy is considered safe when performed by experienced and well-trained gentic scientists following established laboratory protocols.
The procedure involves removing a small number of cells from the outer layer of the embryo, which does not develop into the fetus.
At Sunfert, strict quality control measures and laboratory protocols are followed by all clinical team members, including embryologists and genetic scientists, to ensure the highest standards of embryo safety.